
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Philip L Millstein*, Carlos Eduardo Sabrosa, Wai Yung and Karen Geber
Corresponding Author: Philip L Millstein, Department of Restorative Dentistry, Harvard School of Dental Medicine, Boston, Massachusetts, USA.
Received: December 10, 2025 ; Revised: December 13, 2025 ; Accepted: December 17, 2025 ; Available Online: December 19, 2025
Citation: Millstein PL, Sabrosa CE, Yung W & Geber K. (2025) Immediate Implant Placement and Loading with Restoration in Occlusal Contact. J Oral Health Dent Res, 5(2): 1-4.
Copyrights: ©2025 Millstein PL, Sabrosa CE, Yung W & Geber K. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
This paper describes a means to obtain occlusal contact guidance upon immediate implant placement.
Preliminary occlusal contact is achieved at the time of implant placement
Keywords: Implants, Restoration, Occlusal contact, Placement procedures.
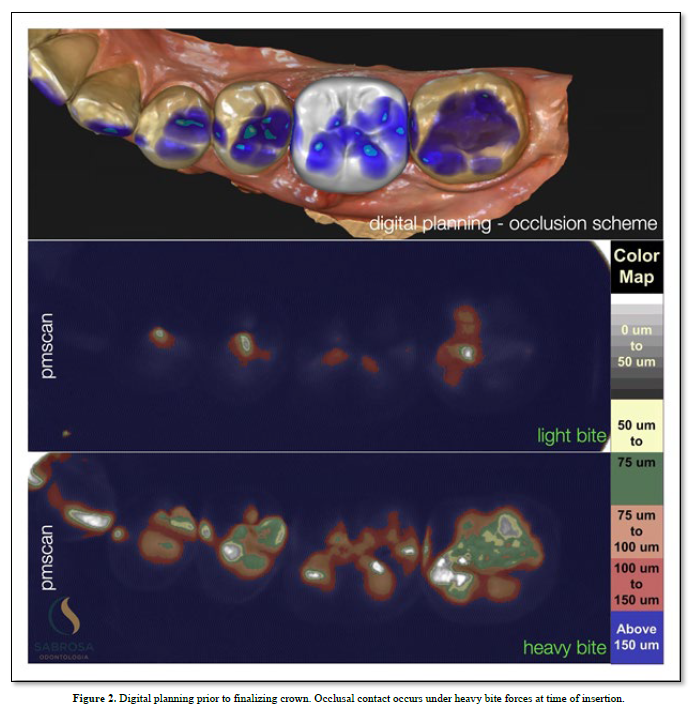
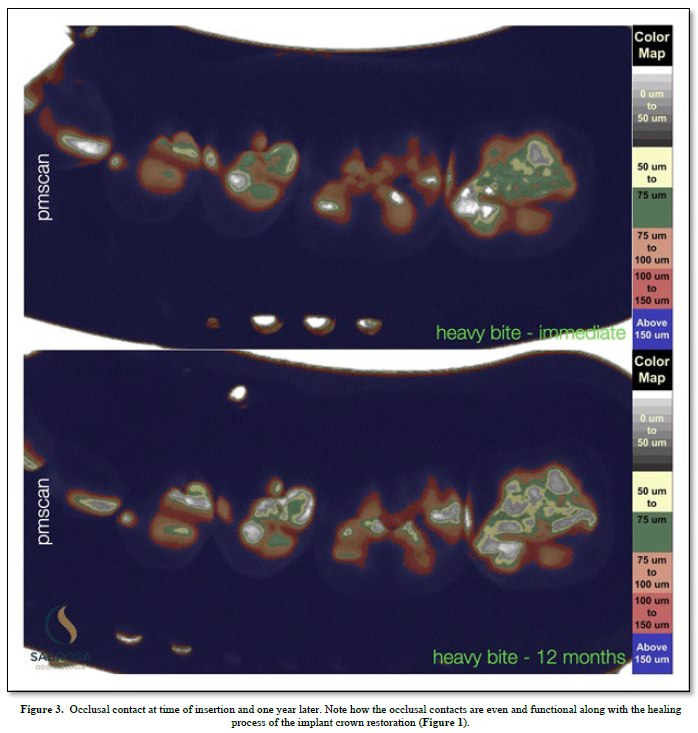
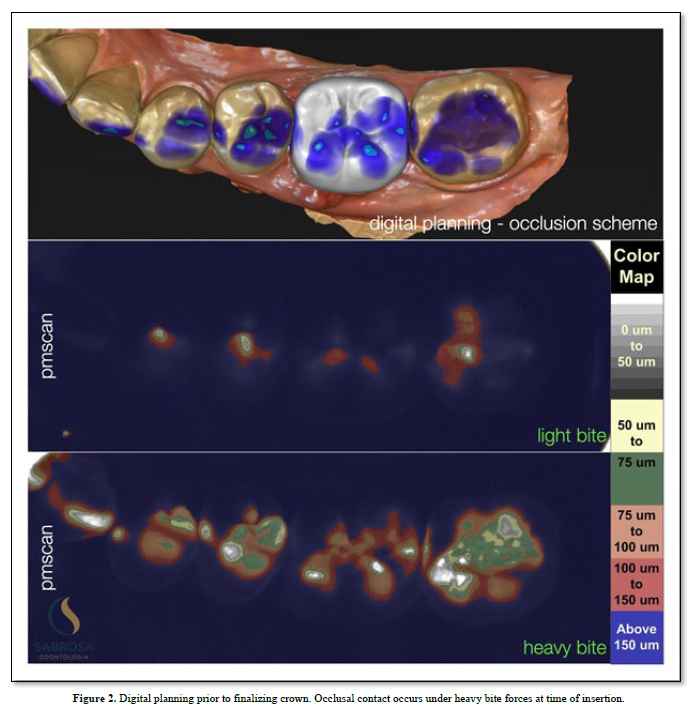
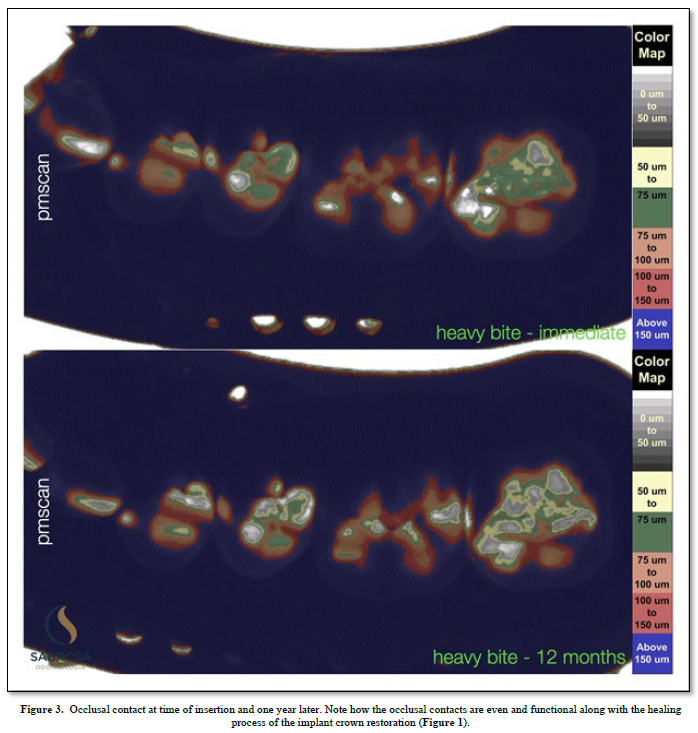
Proprioception is used to navigate space in order for a subject to find a place to make physical contact. (1) An implant with no periodontal housing exhibits little or no proprioception. It has no periodontal housing and no touch or pressure sensors. An opposing functioning tooth with periodontal support is proprioceptive. It is touch sensitive (2). The pressure sensors detect motion and help to reposition and maintain the tooth in a functioning occlusal position. There is little or no information concerning implant proprioception. In a functioning dentition teeth find their position by adjusting to the existing teeth in occlusion. An under occluded implant crown cannot adapt to an existing occlusion without planned occlusal contact guidance. Positional direction and intensity of contact are left to chance. We, as humans, have five senses one of which is touch. Sharks have six senses one of which is touch from a distance (3). Weak electrical signals are used to make contact from afar. Humans can not touch without making physical contact. An implant crown that is under articulated cannot fit into an opposing dentition without making occlusal contact. Total implant placement procedures and restorative healing results are shown (Figure 1). Without implant restorative occlusal contact adjacent teeth and the surrounding dentition adapt to an altered occlusion. Stress distribution is uneven because fewer teeth maintain the occlusal load. Missing limb syndrome where the patient assumes limb retention upon fitting a prosthetic device may be applied to replacing missing teeth where the patient upon tooth replacement immediately assumes past functioning habits. In this case, as shown, tooth and jaw movements related to an altered occlusion are slight but tooth movements are discernible. The occlusal patterns have shifted. There is an uneven amount of occlusal contact upon the second molar (Figure 2). One year later the occlusal contact areas are more evenly distributed. The implant restoration is in functional occlusion. The second molar now fits into the occlusal scheme as does the first molar implant restoration. The teeth have been realigned (Figure 3). In order to plan the occlusion of this implant the clinician (CES) adjusted the surface of the milled zirconia crown (Cerec) prior to completion so that it would just make occlusal contacts upon hard closure (Figure 2). Clinical acumen dictates how much occlusal clearance is required. It is estimated that teeth intrude up to 100 microns upon occlusal loading (3). We assume that when the tooth is fully loaded it will make occlusal contact with its antagonist but when not loaded it will not make contact (4) (Figure 2). To verify contact and non-contact we make a silicone inter occlusal record at the time of insertion (5). The impression is removed and immediately processed using a specially made occlusal scan which includes a direct current light box positioned six inches from an enclosed overhead camera which is connected to an image producing means for recording and interpreting various thicknesses of impression material. The results using image analysis (Image J) can be assessed numerically or viewed using assigned colors that relate to the numbers (6). Two hundred fifty-six pixels is the baseline and the color is white (contact).
A reduction in compressed impression material as shown by using associated colors represents near and far areas of occlusal contact. Proprioception has become a discerning factor. If the implant crown does not have minimal contact upon placement, it may not adjust to the opposing tooth. Proprioception tells your brain where your body parts are located in relation to one another. It works to guide motor skills and to control movements.

An articulation or disarticulation of the jaws occurs when a change in positional occlusal contact takes place. The mandibular position to the maxilla is altered. Force distribution and intensity shift in all teeth. Teeth grind in an attempt to find a stable occlusal position. Every tooth has its own sensory system. Even though occlusal change appears minimal, placing under occluded crowns can be costly to optimum occlusal health. An occlusion which does not include substantial occlusal contact of every functioning tooth is not stable. It will continue to shift. There is no means for self-correction. Clinical intervention is required.


No Files Found




Internationally Accepted
Share Your Publication :